Most of the focus in intervention planning is on the intervention itself: the room, the family, the letters, the moment of confrontation and compassion. However, the 72 hours that follow are just as critical, and it's during this time that many families find themselves unprepared. We've seen successful interventions unravel in the hours after a …

Most of the focus in intervention planning is on the intervention itself: the room, the family, the letters, the moment of confrontation and compassion. However, the 72 hours that follow are just as critical, and it’s during this time that many families find themselves unprepared.
We’ve seen successful interventions unravel in the hours after a loved one agrees to go to treatment, because the logistical and emotional chaos of that period wasn’t anticipated. And we’ve seen families navigate it with grace and effectiveness when they knew what to expect.
Here’s what actually happens after an intervention ends and how to be ready for it.
The First Hour: Momentum Is Everything
When a loved one says yes in an intervention when they agree to go to treatment, that agreement is real, but it is also fragile. The addiction that has been running the show for months or years is still present, and it will begin almost immediately to generate reasons for delay.
“Can I just sleep on it?”
“Let me make a few calls first.”
“I need to take care of a few things before I go.”
“Can I go next week instead?”
These aren’t necessarily bad-faith responses. In many cases, the person means what they’re saying in the moment, and they genuinely want to get help. But the architecture of addiction is designed to find exits, and any gap between “yes” and “departure” is a gap that can be exploited.
This is why we arrange transport in advance. When a loved one agrees to go to treatment in Atlanta, Houston, Phoenix, or San Antonio, the next step is already arranged and waiting. We don’t improvise transportation in the aftermath of a successful intervention. We have it ready.
The goal is to transition from “yes” to “in the car” within two hours whenever possible.
What to Pack, and What Not to Pack
Families often get derailed in this window by the logistics of packing. What does their loved one need? How much? For how long?
Keep it simple. Most residential programs have a list of what’s permitted and what isn’t, and our team will have shared that with families in advance. The general rule is: comfortable personal clothing, toiletries, any required medications with documentation, and nothing that could compromise the program environment (drugs, alcohol, certain electronics).
What families often mistakenly allow that causes problems:
- Phones without restrictions (check the facility’s phone policy most have specific windows for calls in early weeks)
- Excessive cash
- Clothes or items that signal the person still has one foot out the door
What the person actually needs most in the first 72 hours is to arrive, be received by staff, and begin detox or intake without the cognitive load of managing their outside world.
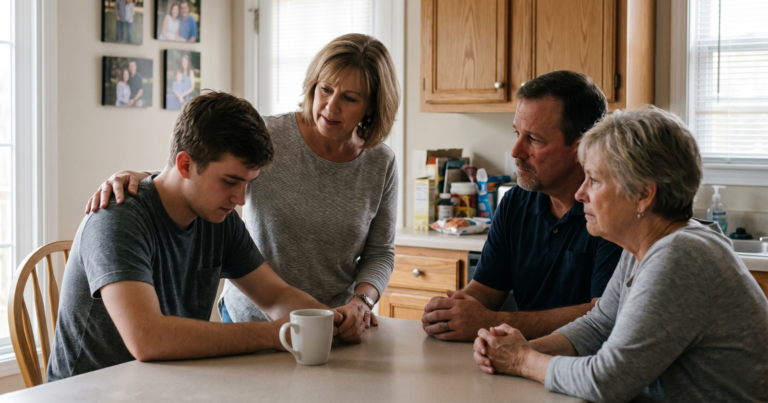
The Goodbye: How to Handle It
For many families, the moment after someone agrees to go, the immediate goodbye before transport, is one of the most emotionally intense moments of the entire process. Parents, spouses, and siblings often don’t know how to act.
A few things our team coaches families through:
Don’t over-explain or re-litigate. The intervention is over. The decision is made. This is not the moment for more processing, more apology, more expression of grievance, or more detailed conversation about what comes next. Brief, warm, simple.
Affirm the decision without making it feel conditional. “I’m so proud of you for doing this” lands differently than “I hope you really mean it this time.” One strengthens the decision. One plants a seed of doubt.
Let them go. This sounds obvious, but it isn’t. Parents especially struggle with the physical act of watching someone they love get in a car and drive away to a facility, potentially far from home. Our interventionists stay present through this moment for exactly that reason.
The First Night: What the Family Experiences
While the loved one is being transported and beginning intake, the family is at home, and the emotional crash can be severe.
The adrenaline of intervention planning, execution, and the immediate aftermath gives way to exhaustion, second-guessing, and a kind of emotional void. “Did we do the right thing?” is almost universal in the first 24 hours, regardless of how clearly the answer is yes.
This is normal. It is not a sign that the intervention was wrong. It is the nervous system coming off a long period of hypervigilance.
Our team remains available to families in this period. We don’t consider our job done when the car door closes. Families in Tennessee, Pennsylvania, South Dakota, and Maine wherever they are, can reach us in those first hours if they need support or have questions.
The First 24–48 Hours: What the Facility Experience Looks Like
Families sometimes don’t know what’s actually happening to their loved one after intake, and that uncertainty increases anxiety. Here’s a general picture:
Medical intake and assessment. The facility will conduct a physical assessment, review medication history, and determine what level of medical supervision is needed for detox. For alcohol, this may involve medication management. For opioids, MAT (medication-assisted treatment) options will be assessed.
Orientation. Most programs have a structured orientation period where new patients are introduced to the environment, the schedule, and the expectations. This is often disorienting, but intentionally so; the structure itself is part of the treatment.
Limited communication. Many facilities have a blackout period of some kind in the first days, limited or no phone contact with family. This is intentional. It allows the person to begin adjusting without the pull of outside voices, including well-meaning family members who may inadvertently undermine the process.
If the facility hasn’t communicated what to expect regarding contact, call the admissions team directly and ask.
What Families Should Do in This Window
The 72 hours after an intervention are a critical reset period for the family, not just the person in treatment.
Start your own support. Al-Anon, family therapy, individual counseling, whatever form it takes, the family system that has been organized around managing someone else’s addiction needs support of its own. This isn’t a side note. It is central to the loved one’s long-term recovery.
Don’t make major decisions. This isn’t the week to have difficult conversations about the relationship, financial arrangements, living situations, or the future. Give the dust a chance to settle.
Communicate simply with others who need to know. You don’t owe anyone an explanation, but if employers, schools, or extended family need to be told something, keep it brief and factual.
The Moment That Feels Like the End Is Actually the Beginning
Every family we’ve worked with has, in the hours and days after a successful intervention, said some version of the same thing: “I can’t believe we actually did it.”
There is a sense of unreality to those first 72 hours. Something that felt impossible for months or years has actually happened. The person they love is in treatment. And yet the fear doesn’t immediately leave, because they know this is just the start of a longer road.
That’s an accurate read. Recovery is a long road. But the hardest part, getting the person into a position where they can start, is done. What comes next is still hard, but it’s a different kind of hard. And you don’t have to navigate it alone.
Whether your family is in Tennessee, Pennsylvania, South Dakota, Maine, Atlanta, Houston, Phoenix, or San Antonio, our team is with you through this, not just for the intervention, but for what comes after.
Book a Consultation
It’s easy and free!