QUICK SUMMARY Texas transferred $11.8M in opioid settlement funds to hospital districts in April 2026 — pushing the state's total past $300M. Here's what that money can and can't do for your family right now. •Overdose deaths remain elevated across all 254 Texas counties — Travis County deaths tripled between 2019 and 2023 •Fentanyl is …
QUICK SUMMARY
Texas transferred $11.8M in opioid settlement funds to hospital districts in April 2026 — pushing the state’s total past $300M. Here’s what that money can and can’t do for your family right now.
- •Overdose deaths remain elevated across all 254 Texas counties — Travis County deaths tripled between 2019 and 2023
- •Fentanyl is being found in pills that look identical to legitimate prescriptions
- •Covers Houston, Dallas, San Antonio, and Austin — each city has a distinct drug and family profile
- •Bexar County has the highest neonatal abstinence syndrome rate in the state
- •ARISE® invitational model: 60%+ enter treatment within the first week — no confrontation, no ambush
- •The 72-hour window after “yes” is the highest-risk point — sober transport and aftercare are critical
- •Settlement funds build infrastructure — they don’t make the call inside your family that has to happen first
On April 6, 2026, the Texas Opioid Abatement Fund Council quietly transferred $11.8 million to hospital districts across the state. It’s the kind of headline most families scroll past. Another big number. Another government check. Another agency saying it’s doing something about the opioid crisis.
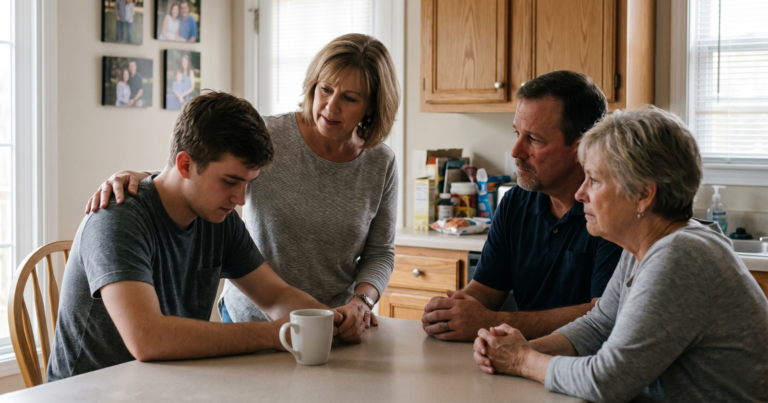
But if your son or daughter or husband or mother is the person you’re worried about tonight, that $11.8 million doesn’t sound like progress. It sounds like noise. Because the gap between a state-level funding announcement and your family actually getting somebody into treatment is enormous, and nobody fills that gap by accident. If you’re searching for a professional intervention in Texas, it’s because you already know the truth: money helps, but it doesn’t show up at your door at 11 p.m. when your loved one finally agrees to talk. Somebody has to.
This piece is for the somebodies. It’s about what that $11.8 million is actually doing, where it falls short, and what a Texas family can do this week if they’ve decided that “we’ll figure it out eventually” is no longer a plan.
What the money is funding, and what it isn’t
The latest disbursement, announced by the Texas Comptroller’s office, pushes the state’s running total of opioid settlement distributions past $300 million. Most of it lands at the county and hospital-district level, where it gets routed into things like medication-assisted treatment expansion, naloxone distribution, neonatal abstinence programs in Bexar County, and crisis services in metro hospitals. That’s good. Those programs save lives every day, and the public-health professionals running them deserve every dollar.
But notice what isn’t on that list. Nobody on a state budget line is going to call your brother. Nobody at the Health and Human Services Commission is going to sit on your living room floor at midnight and help your mother stop covering for him. Nobody from the abatement fund is going to drive your sister to detox in Houston when she finally says yes. Public dollars build the infrastructure. They don’t make the call inside your family that has to happen first.
Texas is also still losing people fast. The state’s Targeted Opioid Response program, funded by SAMHSA, reports that overdose deaths remain elevated across all 254 counties even as the curve has started to bend in some metros. Travis County’s accidental drug deaths roughly tripled between 2019 and 2023. Bexar County still has the highest neonatal abstinence syndrome rate in the state. Fentanyl is showing up in pills that look identical to legitimate prescriptions. The crisis didn’t end. It got quieter and more chemical.
So the question isn’t whether the money is doing something. It is. The question is what your family is going to do with the time the money buys.
The gap nobody’s funding
There’s a part of this story the state can’t fund, no matter how many billions arrive in settlement payments: the moment a family stops protecting the addiction and starts confronting it.
Most families wait too long. Not because they don’t care. They wait because each individual day looks survivable. Yesterday they made it. Today they’ll make it. Tomorrow they’ll talk about it, maybe, when things calm down. But things don’t calm down. They escalate. The CDC’s overdose surveillance data makes it brutally clear: in the fentanyl era, the runway between “manageable problem” and “preventable death” can be a single night. A pill from a friend. A relapse after thirty days clean. A drink at the wrong wedding.
The waiting itself becomes the most expensive thing a family does. And it’s expensive in ways that don’t show up in a settlement account. It’s expensive in trust, in marriages, in younger siblings who learn that the loud one always gets the help. By the time a Texas family contacts a professional interventionist, they’ve usually been in the thick of it for three to seven years.
This is why our team built G3 Recovery the way we did. Both founders, Matt and Hannah Gibson, have lived this from inside. Matt is a Certified ARISE® Interventionist; Hannah is in long-term recovery. They’ve been through the version of this story where nobody knew what to do, and the version where somebody finally did. The difference between those two outcomes wasn’t money. It was a structure for the conversation, a plan for the next forty-eight hours, and a person on the phone who’d done it before. You can read more about the team and the model on the Who We Are page.

What the gap looks like in Texas’s four big metros
The shape of addiction in Texas isn’t uniform. Each major metro has its own version of the same crisis, and the right way in changes accordingly.
In Houston, the dominant story is fentanyl mixed into other substances. Methamphetamine relapses laced with synthetic opioids are sending people to the ER at rates ICUs haven’t seen since the early pandemic years. Families dealing with stimulant use disorders are often the most blindsided when an overdose happens, because they didn’t think their loved one was using opioids at all. If your family is closer to that picture, our team works on drug intervention in Houston and a parallel track for meth intervention in Houston.
In Dallas, alcohol still dominates the calls we take, often layered with prescription benzodiazepines. The Dallas-Fort Worth corporate culture creates a particular kind of high-functioning denial: the person is still going to work, still closing deals, still showing up to family events, and the spiral is invisible until it isn’t. We support those families with alcohol intervention in Dallas and drug intervention in Dallas tracks tuned for high-functioning use.
In San Antonio, where neonatal abstinence syndrome rates are the state’s highest, families are often navigating addiction across two generations at once. A new mother in active use, a partner trying to hold things together, grandparents who never expected to be the primary caregivers. Our San Antonio intervention work is built around these layered family systems, and we coordinate care with the perinatal programs the settlement money is helping to expand.
In Austin, the picture leans younger and more polysubstance. Cocaine, ketamine, fentanyl-laced pills sold as legitimate ADHD medication. The 18-to-30 demographic is overrepresented, and parents are often watching from out of state. We handle these as drug and alcohol interventions in Austin with a tighter focus on treatment placement and family education, since the parents involved usually need a crash course in what their kid is actually using.
The point isn’t that geography determines fate. It’s that the right intervention starts with an honest read of what’s actually happening, not a generic script.
What a real Texas intervention looks like
The Hollywood version of an intervention, surprise circle in the living room, one big confrontation, person breaks down and goes to rehab, isn’t the model that works in 2026. It’s also not the model the Gibsons use. We use the ARISE® Invitational model, which has roughly six decades of clinical evidence behind it and a published outcome of 60% or more of the identified loved one entering treatment within the first week.
Here’s how that actually unfolds in Texas, in plain terms:
A family contacts us. Usually a spouse or a parent. We schedule an initial consultation, often the same day, and we talk through what’s happening, who’s involved, what’s already been tried, what’s making it worse. We map the family system: who’s enabling without realizing it, who’s isolated, who has the leverage, who has the trust.
We invite the loved one to a meeting. Not a surprise. The Invitational model means the person who is using knows the meeting is happening and is invited to join. Most do. The ones who don’t, we still hold the meeting without them, because the family’s healing doesn’t depend on whether the person says yes that day.
We work the framework G3 calls RECLAIM, which is our gather-guide-grow approach: gather the family network, guide the conversation with a structured agenda, and grow the changes through aftercare and continuity. Treatment placement is part of it. So is family consulting, recovery coaching, and, when the moment comes, sober transport in Texas so the loved one actually arrives at treatment instead of disappearing in the parking lot.
Most families are surprised by how non-confrontational the process is. There’s no shouting. There’s no ambush. There’s a structure, and somebody experienced running it, and the structure does the work that families have been trying to do alone for years.
After the yes
A yes is not the end. It’s the start of a new fragility.
The first 72 hours after an addicted person agrees to treatment are statistically the highest-risk window of the entire process. Plans fall apart. Phones get used. Friends show up unannounced. The body’s withdrawal accelerates faster than the family’s logistics. This is where most untrained interventions lose people.
It’s also where professional aftercare matters most. Our recovery coaching and family consulting work picks up the moment treatment placement is confirmed and stays in the picture as long as the family wants. Not as a sales handoff, but as continuity. The Gibsons are in long-term recovery themselves; they know what week three looks like and what month six looks like, and they’ve watched too many families lose somebody in the gap between rehab discharge and “back to normal life.”
What the money can’t fix, and you can
So back to the $11.8 million.
It’s real. It will help. It will fund medications, harm reduction, hospital programs, and family-preservation services that didn’t exist five years ago. Texas is doing more on the opioid crisis than it has in any recent year. That’s worth saying out loud.
But it can’t make the call from your family. That part is still on you.
If you’re somewhere in the deciding part of this, where you’ve watched too many small things and you’re starting to suspect there isn’t going to be a clean window when everything calms down on its own, the most useful thing you can do this week is talk to somebody who has done this before. We’re at (214) 927-2154, or you can start a confidential conversation here. No pressure, no script. Just a real human who has been on both sides of the situation you’re sitting in.
The state’s money is doing its job. Now your family gets to do yours.
Frequently Asked Questions
Is a professional intervention right for my Texas family if my loved one isn’t ready?
Almost nobody is “ready” before an intervention. That’s the whole reason interventions exist. The ARISE® Invitational model is built specifically for situations where a family has been waiting for readiness that isn’t coming. The structure creates the readiness, in most cases within the first week.
How fast can G3 schedule an intervention in Texas?
For most Texas families, an initial consultation happens within 24 to 48 hours of the first call. The intervention itself is typically scheduled within one to two weeks, depending on the family’s logistics and the urgency level we assess on the consult.
Does insurance cover an intervention?
Most insurance plans don’t cover the intervention itself, but they do cover the treatment that follows. Part of our process is helping you understand your insurance benefits and pre-authorize treatment placement before the intervention happens, so the path from “yes” to admission is clear.
What happens if my loved one says no?
Roughly four out of ten people don’t say yes the first day. That doesn’t mean the intervention failed. The Invitational model continues to work in the days and weeks after the first meeting, and the structure gives the family a way to hold healthier boundaries while staying in relationship. A lot of “no” answers turn into “yes” within thirty days.
Are settlement-funded programs in Texas the same as what G3 does?
No. The state-funded programs do critical public-health work: medication access, hospital crisis services, harm reduction. G3 is a private clinical intervention practice. We work with families one-on-one to plan, run, and follow through on interventions and family consulting. The two systems complement each other; they don’t substitute.
Book a Consultation
It’s easy and free!