QUICK SUMMARY California seized $11.4M in fentanyl in Q1 2026 — 1,500 lbs of powder, 700k counterfeit pills. Here's what that means for families still in crisis right now. •LA County overdose deaths dropped 22% in 2024 — fentanyl deaths down 37%, the largest decline in county history •Pills already in circulation aren't recalled — …
QUICK SUMMARY
California seized $11.4M in fentanyl in Q1 2026 — 1,500 lbs of powder, 700k counterfeit pills. Here’s what that means for families still in crisis right now.
- •LA County overdose deaths dropped 22% in 2024 — fentanyl deaths down 37%, the largest decline in county history
- •Pills already in circulation aren’t recalled — the risk at home hasn’t changed this week
- •Covers LA, San Francisco, San Diego, and Sacramento — each city has a distinct drug and family profile
- •ARISE® invitational model: 60%+ enter treatment within the first week — no ambush, no confrontation
- •The 72-hour window after “yes” is the highest-risk point — sober transport and aftercare are critical
- •State programs and G3 are not the same — interdiction and harm reduction don’t replace family-level intervention
G3 Recovery Interventions • professionalinterventions.com • (214) 927-2154
On April 28, 2026, Governor Newsom announced that California’s National Guard Counterdrug Task Force has helped seize more than $11.4 million worth of fentanyl off California streets in just the first three months of the year. Fifteen hundred pounds of powder. Seven hundred thousand counterfeit pills. A single load of that volume is enough to kill, by some estimates, hundreds of millions of people.
Big number. Real win. Worth saying out loud, because California has been losing this fight by a brutal margin for almost a decade. But if you’re a parent in Sacramento or a wife in San Diego or a sibling in the Bay Area, $11.4 million in seized supply doesn’t change the conversation in your kitchen tonight. The pills already out there don’t get vacuumed back. The relapse risk doesn’t pause. Whatever was happening at home before this announcement is still happening this week. If you’re searching for a professional interventionist in California, you already know that. The supply story and the family story aren’t the same story.
This piece is for the families. It’s about what state interdiction actually does, what it can’t do, and what a California family can put in motion this week if they’ve decided that “we’ll figure it out eventually” is no longer a plan.
What the seizures are doing, and what they aren’t
The April announcement, made through the Governor’s office, lays out an interdiction record that’s genuinely meaningful. CalGuard’s task force is now partnering with local law enforcement at a scale California has never run before. March alone produced more than 663 pounds of fentanyl seized and almost 270,000 fentanyl-laced pills taken off the street. That’s supply that won’t reach a kid at a party in Long Beach. It’s pills that won’t end up cut into someone’s Adderall in Berkeley. The lives those seizures buy back are real, even if you can’t name them.
And there’s separate good news on the demand side. Los Angeles County reported a 22 percent decline in drug-related overdose deaths in 2024, including a 37 percent drop in fentanyl deaths. That’s the most significant decline in LA County’s history, and it’s the kind of number public-health teams have been working a decade to produce.
So California is doing something. The trend lines are starting to turn. None of that is in dispute.
What’s in dispute is whether any of that helps your specific family this week.
It doesn’t, directly. Nobody at CalGuard is going to call your son. Nobody at Public Health is going to walk into your daughter’s apartment and say what needs to be said. The pills already in circulation, the patterns already in motion inside someone’s life, the addiction that’s been dug in for three or five or seven years, none of that gets resolved by a press conference. State infrastructure changes the long-term odds. Family action changes this month.
The gap nobody’s funding
Most California families wait too long. Not because they don’t care. They wait because each individual day looks survivable. Yesterday they made it. Today they’ll make it. Tomorrow they’ll talk about it, maybe, when things calm down. But things don’t calm down. They escalate, and in the fentanyl era they escalate faster than families used to plan for. The CDC’s overdose surveillance data shows the runway between “manageable problem” and “preventable death” can collapse to a single night. A pill from a friend. A bump of cocaine that wasn’t just cocaine. A relapse after thirty days clean.
The waiting itself becomes the most expensive thing a family does. And it’s expensive in ways that don’t show up on any state dashboard. It’s expensive in trust, in marriages, in younger siblings who learn that the loud one always gets the help. By the time a California family contacts a professional interventionist, they’ve usually been in the thick of it for three to seven years.
This is why our team built G3 Recovery the way we did. Both founders, Matt and Hannah Gibson, have lived this from inside. Matt is a Certified ARISE® Interventionist; Hannah is in long-term recovery. They’ve been through the version of this story where nobody knew what to do, and the version where somebody finally did. The difference between those two outcomes wasn’t the broader trend lines. It was a structure for the conversation, a plan for the next forty-eight hours, and a person on the phone who’d done it before. You can read more about the team and the model on the Who We Are page.

What the gap looks like in California’s four big metros
The shape of addiction in California isn’t uniform. Each major metro has its own version of the same crisis, and the right way in changes accordingly.
In Los Angeles, the picture is the most visible. Fentanyl-laced pills made to look like Xanax or Percocet are still circulating in social networks where most parents don’t realize their kid is even using anything. The decline in deaths is real, but the underlying use pattern hasn’t dropped at the same rate. Families in LA call us most often when their adult child is using something they think is “safer” than heroin. Our team works on drug intervention in Los Angeles with a parallel track for fentanyl intervention in Los Angeles tuned for the polysubstance reality.
In San Francisco, the public-health response is loud and visible: harm reduction, naloxone everywhere, treatment-on-demand programs in some neighborhoods. The gap families face isn’t access to harm reduction. It’s the gap between harm reduction and abstinence-based recovery for someone who’s tried both. We support those families with alcohol intervention in San Francisco and drug intervention in San Francisco work that pairs medical detox with the family system around the person.
In San Diego, alcohol still drives more of our calls than people expect, often layered with prescription benzodiazepines. The military-adjacent population brings its own complexity: dual diagnosis, PTSD, a culture where the person in trouble has been trained to “handle it.” Our drug intervention in San Diego work is built around those layered systems.
In Sacramento, methamphetamine and fentanyl polysubstance use is showing up in younger demographics than five years ago. Parents are watching from elsewhere in the state and trying to coordinate care across distance. We handle these as alcohol intervention in Sacramento and meth-specific work, with a tighter focus on treatment placement and family education.
The point isn’t that geography determines fate. It’s that the right intervention starts with an honest read of what’s actually happening, not a generic script.
What a real California intervention looks like
The Hollywood version of an intervention, surprise circle in the living room, one big confrontation, person breaks down and goes to rehab, isn’t the model that works in 2026. It’s also not the model the Gibsons use. We use the ARISE® Invitational model, which has roughly six decades of clinical evidence behind it and a published outcome of 60 percent or more of the identified loved one entering treatment within the first week.
Here’s how that actually unfolds in California, in plain terms:
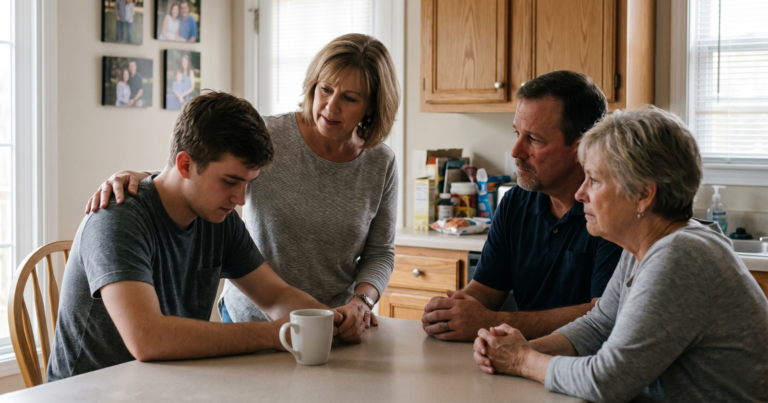
A family contacts us. Usually a spouse or a parent. We schedule an initial consultation, often the same day, and we talk through what’s happening, who’s involved, what’s already been tried, what’s making it worse. We map the family system: who’s enabling without realizing it, who’s isolated, who has the leverage, who has the trust.
We invite the loved one to a meeting. Not a surprise. The Invitational model means the person who is using knows the meeting is happening and is invited to join. Most do. The ones who don’t, we still hold the meeting without them, because the family’s healing doesn’t depend on whether the person says yes that day.
We work the framework G3 calls RECLAIM, our gather-guide-grow approach: gather the family network, guide the conversation with a structured agenda, and grow the changes through aftercare and continuity. Treatment placement is part of it. So is family consulting, recovery coaching, and, when the moment comes, sober transport in California so the loved one actually arrives at treatment instead of disappearing in the parking lot.
Most families are surprised by how non-confrontational the process is. There’s no shouting. There’s no ambush. There’s a structure, and somebody experienced running it, and the structure does the work that families have been trying to do alone for years.
After the yes
A yes is not the end. It’s the start of a new fragility.
The first 72 hours after a person agrees to treatment are statistically the highest-risk window of the entire process. Plans fall apart. Phones get used. Friends show up unannounced. The body’s withdrawal accelerates faster than the family’s logistics. This is where most untrained interventions lose people.
It’s also where professional aftercare matters most. Our recovery coaching and family consulting work picks up the moment treatment placement is confirmed and stays in the picture as long as the family wants. Not as a sales handoff, but as continuity. The Gibsons are in long-term recovery themselves; they know what week three looks like and what month six looks like, and they’ve watched too many families lose somebody in the gap between rehab discharge and “back to normal life.”
What the seizures can’t fix, and you can
So back to the $11.4 million.
It’s real. It will help. CalGuard’s interdiction work, paired with the LA County numbers and the broader state response, is bending a curve that bent in the wrong direction for a long time. California is doing more on this than it has in any recent year. That’s worth saying out loud.
But it can’t make the call from your family. That part is still on you.
If you’re in the deciding part of this, where you’ve watched too many small things and you’re starting to suspect there isn’t going to be a clean window when everything calms down on its own, the most useful thing you can do this week is talk to somebody who has done this before. We’re at (214) 927-2154, or you can start a confidential conversation here. No pressure, no script. Just a real human who has been on both sides of the situation you’re sitting in.
The state’s interdiction is doing its job. Now your family gets to do yours.
Frequently Asked Questions
Is a professional intervention right for my California family if my loved one isn’t ready?
Almost nobody is “ready” before an intervention. That’s the whole reason interventions exist. The ARISE® Invitational model is built specifically for situations where a family has been waiting for readiness that isn’t coming. The structure creates the readiness, in most cases within the first week.
How fast can G3 schedule an intervention in California?
For most California families, an initial consultation happens within 24 to 48 hours of the first call. The intervention itself is typically scheduled within one to two weeks, depending on the family’s logistics and the urgency level we assess on the consult.
Does insurance cover an intervention?
Most insurance plans don’t cover the intervention itself, but they do cover the treatment that follows. Part of our process is helping you understand your insurance benefits and pre-authorize treatment placement before the intervention happens, so the path from “yes” to admission is clear.
Has the recent decline in California overdose deaths changed how you approach interventions?
Public-health gains haven’t changed our model, but they have changed the conversation we have with families. We talk more openly now about the long-term odds being better than they were five years ago. The short-term odds for a specific person in active use, though, haven’t shifted as much. We still treat every call as urgent.
Are state-funded programs in California the same as what G3 does?
No. The state-funded programs do critical public-health work: medication access, harm reduction, treatment-on-demand in some areas, interdiction. G3 is a private clinical intervention practice. We work with families one-on-one to plan, run, and follow through on interventions and family consulting. The two systems complement each other; they don’t substitute.
Book a Consultation
It’s easy and free!